
The floor of the Bank of Oklahoma Center in Tulsa was awash in red, white, and blue. Eager supporters of President Donald Trump were holding signs, wearing “Make America Great Again” hats, and sporting T-shirts with expressions ranging from “Guns, God, and Trump” to “Make Liberals Cry Again.” The attendees were young and old but mostly white. Parents brought their children. There were memorabilia for purchase. Everyone inside the arena had their cell phones at the ready, eager to capture moments of the man of the hour.
Inside, it felt like a typical Trump rally. Outside, however, the atmosphere was tense. It was less than a month since George Floyd had been murdered by Minneapolis police office Derek Chauvin, and protesters had mobilized outside the venue carrying signs that read “Dump the Trump,” “No Justice. No Peace,” and “Defund the Police.” Law enforcement was keeping a tight perimeter. Police brandished shields and clubs, and members of the Oklahoma Highway Patrol and National Guard were armed and ready. On the street—in big yellow capital letters—was written “BLACK LIVES MATTER.”
But it was not just the presence of protestors that made the rally notable. What was truly exceptional was the timing. It was June 20, 2020, and Trump was having his first in-person campaign rally in four months—in the middle of a global pandemic.
In a typical election year, it would be unheard of for a president to take a four-month break from the campaign trail. This is particularly true for a candidate such as Trump who thrives on crowd applause. But this wasn’t a typical year. The United States was in the middle of a global pandemic. The novel coronavirus SARS-CoV-2—commonly known as COVID-19—grew from an infection of zoonotic origin in Wuhan, China, in late 2019 into a public health emergency of global proportions. COVID-19 spreads through respiratory droplets produced when a person breathes, coughs, sings, sneezes, or speaks, and transmission is more likely when people are in close contact with one another, particularly when airflow is poor such as in indoor facilities. COVID-19 infections vary dramatically from person to person. Some carriers are asymptomatic; some experience fever, loss of smell and taste, and shortness of breath; and some end up hospitalized on respirators. And for millions, COVID-19 has proved fatal. The first death from COVID-19 in the United States was recorded on February 29, 2020. By the time of the June 20 rally in Tulsa, that number had reached 115,000 Americans. And by December 2021, over 800,000 Americans had died of COVID-19–related illnesses.
But you wouldn’t know the country was in the throes of a public health emergency by looking at pictures from June 20. Almost everyone in the arena was unmasked, and there was no social distancing. Public health officials and experts had warned the campaign against holding an indoor rally, as COVID cases continued to climb in Oklahoma. But here were more than six thousand Trump supporters, coming out to see their president.1 It wasn’t a full house—the arena was only a third full—but Trump was back on the road as if the pandemic was over. During his remarks, he even quipped that unlike him, his Democratic opponent, former vice president Joe Biden, “remains silent in his basement.” Biden was like millions of Americans: still at home, still socially distancing, still working online, and still navigating the real uncertainty of life during a pandemic.
Trump’s Tulsa rally was a spectacle designed to project strength and “business as usual,” confidently flouting public health recommendations and the commonsense precautions adopted by hundreds of millions of Americans during the pandemic. Biden eventually resumed campaigning but only in socially distanced parking lot events, while Trump kept up his in-person rallies, oftentimes held indoors. Republicans even tried to hold a traditional in-person national convention in Charlotte, North Carolina, but were forced to scale back to a hybrid format when the state government refused to allow the event to proceed at full capacity and without face masks.2
Tulsa and over a dozen similar campaign events held after would come to be described as “superspreader” events. Eight Trump campaign staffers tested positive for COVID after the rally,3 and Tulsa health officials noted the rally “likely contributed” to a surge in new COVID cases.4 One study estimated the collateral effect of these Trump superspreader events: nearly 30,000 confirmed COVID-19 cases, likely leading to more than 700 deaths.5 Trump himself even became a vector. According to White House chief of staff Mark Meadows, Trump tested positive for COVID-19 on September 26, 2020. He then kept up an active campaign schedule for almost a week, knowingly exposing more than 500 people—from fundraisers to staff to Gold Star families to Democratic candidate Biden at the presidential debate in Cleveland, Ohio—before being hospitalized at Walter Reed National Medical Center on October 2.6 Trump received cutting-edge experimental treatment and walked out of the hospital three days later. Upon returning to the White House, he was photographed immediately removing his mask with a still-active case of COVID-19 in the presence of White House staff. He tweeted “Don’t be afraid of Covid . . . Don’t let it dominate your life . . . I feel better than I did 20 years ago!” The same could not be said for the more than 210,000 Americans who had died by that point.
Politicizing a Pandemic
It is difficult to describe the devastation that the COVID-19 pandemic has wrought in the United States. Rich and poor, red states and blue states, Black and white, coastal and inland, metropolitan and rural—no corner of America was unaffected. The first known deaths occurred in mid-February in Santa Clara County, California.7 In March 2020 alone, more Americans died from COVID-19 than the number killed in the September 11 terrorist attacks. By the end of April, the death toll surpassed the number of U.S. military personnel who died during the Vietnam War. By December 2020, at around three thousand deaths per day, each day was a 9/11. By June 2021 when just over half of Americans had received at least their first dose of a COVID-19 vaccine, the total number of deaths had passed six hundred thousand. By December 2021, this grim figure passed eight hundred thousand. Even with a vaccine widely available, the United States was still seeing thousands of deaths per week during the last months of 2021—a figure that far exceeds the death toll from the seasonal flu.8
The catastrophic death toll of the COVID-19 pandemic in the United States was not inevitable. The novel coronavirus strain—SARS-CoV-2, which came to be called COVID-19 (CO for corona, VI for virus, D for disease, and 19 for the year in which it was first identified)—proved novel in more ways than one. Biologically, it was a deadlier strain of the generic coronavirus. It was also novel in the scope and rate of spread. From the first identified case in Wuhan in December 2019, it spread globally in just weeks. Although deadlier diseases such as SARS and Ebola had seen outbreaks in the previous decades, the scale of the COVID-19 pandemic was unequal to any health crisis in recent memory.
And COVID-19 was particularly novel as a public health emergency. Health is not an inherently polarizing issue—everyone wants to be healthy and for their families to be safe. Diseases such as Alzheimer’s, opioid addiction, and cancer do not differentiate between Americans based on their sport allegiances, musical tastes, or partisan preferences.9 When polio was paralyzing and killing children in the United States, Americans across the political spectrum sent three million dimes to the White House and helped fund a polio vaccine.10 And during a public health crisis such as a pandemic, we might expect our differences to fall away as people seek out information about what is happening and how to be safe.11 In the case of COVID-19, that did not happen.
Moreover, as the scale of the crisis became clear, we might have expected that people would pull together to support swift government action to overcome it. Economic crises such as the Great Depression (1929–1933) and the Great Recession (2007–2009) created massive public demand for policies that expanded the scope and size of the federal government to protect citizens from the worst of the financial fallout. Terrorist attacks and military crises have historically increased presidential approval as feelings of solidarity and patriotism grow and criticism from opponents fall away.12 Nowhere was this rally-round-the-flag effect more apparent than after the 9/11 attacks, when “United We Stand” banners hung in American homes and George W. Bush’s approval ratings climbed to over 90 percent.13 This coming together, in the case of COVID-19, did not happen either.
The pandemic in the United States was always going to be bad. We can think of the United States as a medical patient with a set of preexisting conditions that make them susceptible to illness. One preexisting condition was a decaying health care system in which insurance company interests played an outsized role in costs and coverage. A second preexisting condition was deep social, economic, and racial divisions that, combined with unequal access to health care, perpetuated structural inequality. The third preexisting condition was President Trump, obsessed with projecting strength to ensure his own reelection, gutting bureaucracies tasked with coordinating emergency responses, refusing to take responsibility for managing the crisis, and nurturing a cult of personality that revolved around his unchallenged authority.
But nothing proved more consequential for deepening the COVID-19 crisis than the fatal comorbidity of partisan polarization. Polarization refers to a tendency of parties, movements, and individuals to locate themselves on the extremes of a political spectrum rather than in the center. It is the “simultaneous presence of opposing or conflicting principles, tendencies, or points of view.”14 Democracy is inherently conflictual and competitive, but polarization distances people from one another, reducing the potential for consensus and, in its extreme form, civility. As political scientists Jennifer McCoy and Murat Somer write, “polarizing politics always carries the risk of taking on a life of its own, eviscerating cross-cutting ties and nonpartisan channels for compromise, and becoming pernicious.”15
In short, polarization divides the “we” of “we the people” into an “us” versus “them.” Individuals flee the center, where cross-group dialogue and compromise take place, and move to the extremes. And in the United States, this centrifugal force is powered by partisanship. Two parties—Democrats and Republicans—divide the American electorate.
In the United States today, partisanship is not merely the candidate you choose or the policies you support. Partisanship in America is a social identity. It is a suite of opinions, experiences, and characteristics that define not just who you vote for16 but also, increasingly, who you are. Importantly, partisanship is a social identity because it is not just about how you feel individually but also how you present yourself and relate to others, both those who hold the same partisan identity as you (your copartisans) and those who do not (your partisan opponents).
Of course, individuals hold many social identities, including gender, religion, class, education, and personality. But in the United States today, many of these identities are becoming aligned with partisanship.17 Historically, for example, observant Christians in the United States were core constituencies of both the Republican and Democratic parties. Today, white evangelical Christians overwhelmingly vote for Republicans.18 Rural Americans have historically voted for both Republicans and Democrats, but today rural whites increasingly align with the Republican Party.19 For these reasons, political scientist Lilliana Mason describes partisanship as a “mega-identity, with all the psychological and behavioral magnifications that implies.”20
When partisanship is a social identity, it connects the idea of who is a Democrat or Republican to what Democrats or Republicans do and who they listen to. For instance, if Americans approached partisanship programmatically—that is, by examining the issues they cared about and seeing which party best espouses them—voters would abandon their partisan identity when parties changed their positions. But rather than change or update their partisanship when parties change positions, strong partisans (that is, those who strongly identify with one party) change their positions to match the party with which they identify.21 There is no better evidence for this proposition than the norm-shattering experience of the 2016 presidential election. The Republican Party, long viewed as the party of American global capitalism, found itself led by a politician who railed against global trade and in favor of protectionism. Once the party changed, so did the preferences of many of its supporters. In other words, Americans remained loyal to their partisan identity rather than to their policy beliefs. This is what political scientist Julia Azari notes is the toxic combination of “weak parties and strong partisanship,” the willingness of party members to follow a president and party even as they move away from core principles.22
American politics has not always been characterized by extreme partisan polarization. The country’s winner-take-all electoral system produces a two-party system in which both Republicans and Democrats must appeal to multiple social groups to form a viable electoral coalition. But whereas once there were ideological differences within parties (e.g., conservative Democrats, liberal Republicans), ideology now so closely aligns with partisanship that liberals vote for Democrats and conservatives vote for Republicans. Even most independents lean toward one party or another and behave in ways that resemble partisans.23
Citizens are good at taking party cues because Americans have sorted into partisan social groups that bring their social identities in line with their partisan affiliations.24 Take again the example of rural white Americans. The process by which rural whites have become a bedrock Republican constituency has two implications. First, rural whites may no longer know anyone who is also a rural white but who is not a Republican. In previous eras, Americans’ social worlds included both Democrats and Republicans even if they were all of the same economic or occupational background. These cross-cutting social ties were once a key factor in undermining partisan divisions in American society but are now less common and more tenuous.25 Whereas common social and economic bonds once overrode partisan divisions, today Americans on the Left and the Right just do not interact as much as they used to.
The second implication of partisan sorting is more ominous. If partisanship is a “mega-identity” that increasingly aligns with other social identities, then it follows that one can mobilize partisans without appealing to partisanship itself. A campaign that is relatively certain that rural whites share its partisan orientations is just as effective in mobilizing their votes by appealing to their rural or white identity as by appealing to their views on agricultural policy. This also incentivizes politicians to use messages targeted at specific group identities rather than messages that appeal across groups.
Therefore, in the same way that we often hear about red states and blue states, we can think of “red” and “blue” Americans. These aren’t just words that describe one’s politics; instead, they capture a way of life. For instance, during a colorful interview between Michael Anton, a former Trump national security official, and National Public Radio host Steve Inskeep, Anton identified himself as a “red person” who had formerly been a “blue person.”26 A blue person might listen to National Public Radio, drive a Subaru, recycle, watch independent films, support pro-choice politics, and live in a blue state. A red person might drive a truck, watch Fox News, attend an evangelical Christian church, and support Blue Lives Matter. And, as it turns out, red and blue Americans respond differently to a pandemic.
Deep partisan polarization created two pandemic realities in America: one where the pandemic was taken seriously and one where the pandemic was an inconvenience. For many Americans the pandemic meant washing hands, wearing masks, avoiding contact with loved ones, canceling travel, and waiting for a safe vaccine or a proven treatment. For others the pandemic was overblown, mostly a problem for the old and infirm similar to the seasonal flu and certainly not a virus that would require major changes to how Americans lived. Many among this group were skeptical of science and vulnerable to misinformation about the virus and vaccines. The consequences have been tragic, as those who ignore public health guidance have become particularly vulnerable to falling victim to the coronavirus themselves, thus prolonging the pandemic.
When it comes to a communicable virus that requires collective action, partisan polarization undermines a government’s ability to respond effectively. At the highest levels of government, polarization made the federal response slower and less effective. Polarization determined which states would receive federal aid, on what terms states would mitigate viral spread, and which children would attend school in person or online. It determined which experts to listen to and who citizens should trust. It determined who wore masks and who did not. It fostered an environment of low trust in government and in each other. In total, partisan polarization produced a public response to the pandemic in which individuals assessed risks, formulated attitudes, and participated in certain health-related behaviors (or not) because of their party identification.
But this was not inevitable. Yes, America faced difficult structural and social preconditions that would make any pandemic hard. Yes, Americans were sharply divided by partisanship at the outset of the crisis. But polarization is not an inevitable barrier to collective action or to a coordinated, effective response to a pandemic. Partisan and other forms of polarization are common around the world,27 and deeply divided countries such as the United Kingdom, South Korea, and Taiwan did not make partisanship the lens through which to see or experience the COVID-19 pandemic. Partisan divisions may be deeper and wider in the United States than in any other advanced democracy,28 but this did not make their manifestation in response to COVID-19—over issues ranging from perceptions of the government’s handling of the crisis to mask wearing and contact tracing—inevitable.
The crucial factor that differentiates the United States from other high-income democracies is that the Trump administration chose to make the pandemic political. In the early days of COVID-19, there was a cacophony of conflicting messages, both within and between the scientific community and politicians, as politicians were figuring out what to do and as scientists continued to learn what the virus was and how it evolved. When people are concerned about health crises, they usually trust medical experts more than political leaders and want to hear from them.29 These early days were the window of opportunity during which political leaders faced a choice: they could put experts out front and center and assemble a united, bipartisan strategy to combat the virus, or they could choose to exploit partisanship, activating political divisions to further their individual and partisan goals. The Trump administration chose partisanship.
What does it mean to “choose partisanship?” America’s national leaders chose to preserve a strong economy in an election year, chose an image of strength over the potentially worrisome look of mobilizing resources early, and chose not to encourage deference to trusted public health leaders. Instead, the president and conservative media publicly and repeatedly disagreed with public health experts about how serious the coronavirus pandemic was and what types of policies could effectively manage it.30 The active undermining of experts began with the president, seeped into agencies over which he had significant influence such as the Centers for Disease Control and Prevention, was amplified by conservative media outlets, and trickled down to state governors and mayors. And most of all, it influenced the behavior of the millions of Americans who looked to him for leadership.
Having multiple conflicting messages—and an executive who undercuts his own health bureaucracy—meant that Americans had to decide about how to evaluate the threat from the coronavirus and subsequently how to react. Given these conflicting cues, Americans listened to the leaders of their parties. This led to sharp partisan differences in the ways that ordinary Americans responded to the crisis.
This is our argument. The core explanation for America’s disastrous response to COVID-19 is partisanship. The Trump administration and its partisan allies chose to politicize the pandemic by associating it with Trump’s own fate in office. That decision cast the subsequent response to the COVID-19 pandemic as primarily about partisan politics rather than public health. This partisan response was all-encompassing, touching everything that the pandemic touched, from health behavior to policy views to worries about the election that occurred during the pandemic’s peak. And as these differences persisted, they metastasized. Partisanship undermined Americans’ social solidarity—their willingness to adopt behaviors to protect others and sometimes themselves—and became the core framework through which Americans interpreted and elected officials reacted to the pandemic. Those differences in opinions and the differences in the behaviors that follows have cost hundreds of thousands of American lives. And after two years of pandemic politics the policy landscape is forever changed, as formerly bipartisan issues—such as measles and polio vaccine requirements for schoolchildren and trust in experts—are now politicized like never before.
Surveying a Pandemic
Why did California and Nevada issue stay-at-home orders but neighboring Utah and Wyoming did not? Why was the president of the United States telling Americans that COVID “will go away. Just stay calm. It will go away” while hospitals were at capacity and nurses and essential workers protested outside for protective gear such as face masks? Should we be wiping down our mail with disinfectant? Can I see my neighbor if we’re outside and socially distant? Where can I buy toilet paper? Should I wear a mask outside? Are we flattening the curve? How much longer are we supposed to work from home while also supervising our kids in online school? Do you think we’re going to have to cancel our summer vacation? Is the government doing all it can to protect me, my family, and my community?
These are questions that we, like all Americans, started to ask in March 2020. As large segments of American economic and social life moved online and at home, we also saw our lives overturned by the force of the pandemic. As political scientists, we were specifically attuned to observing the politics of this shift. And as specialists in political processes and behavior—both in the United States and around the globe—we were paying attention to political information and how our fellow Americans were reacting to it. Despite the suggestion that it “will go away,” the early stories of mounting caseloads, overrun hospitals, quarantined citizens, and lockdowns coming out of China and Italy were impossible to ignore.
Recognizing the inevitability of COVID-19 reaching the United States, we decided to pool our skills to study American attitudes and behaviors. Each of us is an expert in a different field of politics: emotions and external threat from terrorism to health scares, mostly in the United States (Gadarian); citizenship and democratic threat, including immigration and electoral interference, mostly in Europe (Goodman); and economic crises and democratic backsliding, mostly in Asia (Pepinsky). Our areas of interest and our existential worries started to blend into the same conversation. We wanted to know who in America shared our worries. We wanted to know if Americans would rally together to fight this collective challenge, or if—as we fearfully suspected from years of research—politics would dominate the U.S. response. And we realized that we could provide a view of the emerging crisis that did not come from the echo chamber of social media or the cacophony of cable news.
Ramping up a large research project to survey Americans on their behaviors and attitudes in response to an emerging health crisis is no small task. Social scientists at federally funded universities are unlike researchers at think tanks and polling firms in that our research plans need to be approved by in-house ethics review committees. In addition, university researchers need to independently obtain funding and coordinate with a contracted survey company to draft up a list of questions. This survey then needed to go into the field, that is, out to our survey respondents. We did all of this in the first two weeks of March 2020. We even wrote down our theoretical expectations about what we thought we might find—specifically, that we would see partisan differences in COVID-19 attitudes and behaviors—and shared them in a public repository. In social science, this is referred to as “preregistering” our research and analysis and is used to increase credibility and reduce hindsight bias. With approval from our ethics boards and emergency funding from the National Science Foundation in a Rapid Response Research Grant, our first survey of Americans launched on March 20 as we ourselves were transitioning to working from home and our kids began learning remotely.
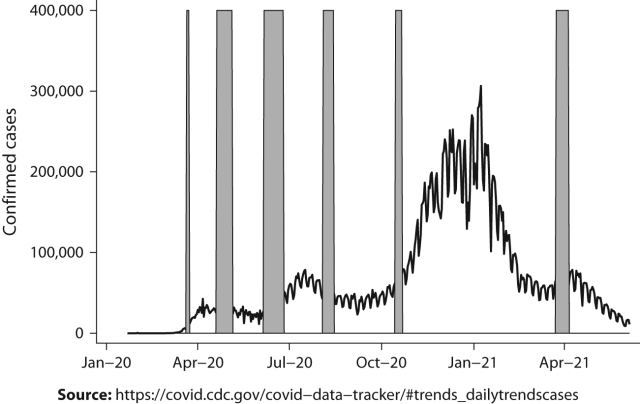
In all, we surveyed ordinary Americans six times, from March 2020 (as states started to lock down, with schools moving to virtual formats and mass cancellation of events) to March/April 2021 (after the inauguration of President Joe Biden and alongside a mass rollout of COVID vaccines). Each wave gives us a different snapshot of America as the pandemic waxed and waned (see figure I.1). We were also able to tap into other events capturing the American public over the year. We could ask questions about, for example, racial justice following the murder of George Floyd (wave 3), the challenges of reopening schools (wave 4), the stakes of the upcoming presidential election (wave 5), and attitudes about vaccines (wave 6). An astute reader might look at this figure and question why we did not have a survey in the field during the peak of the pandemic. For us, the most critical time period was capturing attitudes before the election (wave 5) and after inauguration (wave 6) to see if a partisan change in power produced shifts in policy support or government trust.
At a basic level, our surveys are similar to the standard public opinion surveys released as part of the election cycle. They are designed to be nationally representative, meaning that respondents are chosen randomly but in ways that ensure they reflect, more or less, all adult Americans. This is important: because our respondents are a random but representative sample of all Americans, we can use our surveys to infer what the American population at large was thinking throughout the pandemic. The idea that a survey sample can be representative of a larger population is the bedrock of public opinion research, and we follow this logic as well.
That said, our surveys differ from the standard election poll in two notable ways. First, they are much larger than standard samples: we started with three thousand survey respondents in March 2020, which is about three times as many respondents as we find in most polls. This gives us a great deal of what statisticians call “statistical power,” the ability to identify differences among groups of Americans with a high degree of precision. Smaller surveys can give us an overview of all Americans but might not be powerful enough to detect how subgroups of Americans differ—for example, how attitudes might differ by income, race, or religion. To explore the complexity of Americans’ political responses to COVID-19, we need to collect data on more Americans.
Second, unlike standard election polls, our surveys follow the same individuals over time. This is known as a panel survey design. Public opinion research firms normally draw a sample of, say, 1,000 Americans to conduct a poll, and then when they want to conduct another poll, they draw a new sample of 1,000 Americans. Our strategy was to recontact the same people we polled in the first round every time we conducted a new survey round. In this book, we call each of the rounds of surveys a survey wave, and our respondents whom we interview multiple times are our panel of respondents. Following the same individuals in a panel survey is more costly and time-consuming than drawing a fresh sample for each wave, as the survey firm has to recontact the same individuals and incentivize participation. However, this strategy gives us unparalleled insights into such things as the rigidity or flexibility of beliefs as well as the effect of contextual (e.g., local COVID caseload) or circumstantial (e.g., becoming unemployed) factors over time. In the last survey wave in March/April 2021 (supported by a grant from the Russell Sage Foundation), we added what is called an “oversample” whereby we interviewed an additional set of nonwhite respondents outside of our panel, including 450 Black respondents, 450 Asian American respondents, and 450 Hispanic respondents. These additional respondents allow us to more reliably understand how minority communities fared during the pandemic and what their experiences were with vaccines.
Our Roadmap
In tracing the evolution of health behaviors, attitudes, worries, and policy preferences over the course of the pandemic, we illustrate the early and persistent role of partisanship in shaping individual responses to COVID-19. Despite rising caseloads, uncontrolled spread, and unprecedented loss of life, even taking into account localized factors in an attempt to move away from the national context, partisanship defined both elite and mass responses to the pandemic early on. Once set, the partisan course of the pandemic never deviated.
We develop this argument over ten chapters. Our goal is to produce a definitive account of the politics of the COVID-19 pandemic in the United States, from how it became partisan to the consequences of that choice and from individual worries and policy attitudes to health-related behaviors such as wearing a mask and getting vaccinated. A comprehensive account necessarily begins before the pandemic reached American shores. Chapter 1 sets the stage by describing in detail what we have labeled “preexisting conditions,” which we foreshadowed in this introduction. They include a decaying and politicized health care environment, economic and racial inequality, Trump himself, and, above all, partisan polarization. We think of these conditions as time zero, what epidemiologists would describe as the time before an outbreak threshold when a pathogen starts reproducing at high rates.31 While these factors would make the U.S. outbreak bad, the choice to politicize the pandemic—attaching partisan identity to behaviors and attitudes—made it uniquely worse. Each of these factors on their own would challenge a collective or effective pandemic response; their interaction proved deadly.
Chapter 2 details the onset of the pandemic from January until April 2020. While covering only a short period of time in the long arc of the COVID-19 pandemic, we argue that elite cues, media amplification, and partisan choices in these early critical days were sufficient to permanently affect the trajectory and severity of the pandemic. The series of choices that follow—from early reopenings in the summer of 2020 to Trump rejecting the image of mask wearing even after he became sick with COVID and including differential endorsements and rates of vaccination in red versus blue states—would replicate these early elite patterns. In detailing how the COVID-19 pandemic began to rip through America’s communities, we also see how the interaction of preexisting conditions made the American pandemic uniquely worse. Here we draw a number of comparisons to other countries, from the United Kingdom to Brazil, to illustrate how preexisting conditions such as populist leaders and polarization would make for a bad pandemic, but none make partisan politicization inevitable.
Chapters 3 through 10 move from elites and micropolitics to the focus of our analysis: individuals. The partisan pandemic was all-encompassing—it affected social, economic, and political attitudes. But it begins with health. In Chapter 3, we ask about basic health behaviors. Who washed their hands more often? Who wore masks? Who stopped traveling? Partisanship was consistently the strongest predictor of these health behaviors; specifically, Democrats exhibited more prohealth behaviors than Republicans. Chapter 4 moves to Americans’ worries about the pandemic and the role that emotions play in health behavior and blame attribution. In focusing on these emotional motivations, we see Democrats expressing anger, disgust, and anxiety and more often seeking out information, while Republicans consistently report feeling hopeful.
Chapters 5 through 7 move from individual behavior and emotions to policy attitudes. Chapter 5 begins with health policy: Should the government enforce lockdown measures? Should the government monitor people’s movements? Chapter 6 shifts focus to the economy: What effect did COVID-19 and the economic shutdown have on our respondents? How did experiences such as unemployment affect attitudes about economic policy and government priorities? What should the government do about the economic distress of millions of Americans? Chapter 7 considers immigration policy: Who supports the closure of international borders? Who supports the quarantining of Americans? In each of these policy domains, attitudes strongly divide by partisanship along almost every dimension.
Chapters 8 and 9 situate the pandemic within the context of broader social issues. The pandemic coincided with two of this century’s most significant threats to the United States as a liberal democracy: the exposure of rife racial inequality and police brutality in the wake of the murder of George Floyd, and the contested 2020 presidential election. Chapter 8 examines the intersection of the pandemic and race, exposing and raising awareness of the deep inequality in illness and death experienced by Black and other minoritized American communities. This chapter also explores violence against Asian American communities who were unfairly scapegoated as vectors of infection, an injustice that immigrant communities and their descendants often experience during pandemics.32
Just as equality of citizens is a core tenet of democracy, so are free and fair elections. Chapter 9 looks at the direct assaults on the integrity and independence of the U.S. electoral system. From unfounded concerns about illegal voters to the reliability of vote by mail, American democracy entered the pandemic on precarious footing, but these claims and conspiracies made it worse. By the time Trump-supporting insurrectionists stormed the U.S. Capitol on January 6, deep wounds had already been inflicted.
Chapter 10 closes out the empirical chapters by turning to the politics of vaccination. Policy experts—and millions of eager Americans—optimistically hoped that the arrival of vaccines would usher in the end of the pandemic. Yet, conservative media figures, antivaccination activists, misinformation campaigns, and enduring holdouts had other plans. In looking at vaccine hesitancy, availability, and incentives, we again see how partisanship shaped vaccine uptake. Failing to reach herd immunity by President Biden’s July 4, 2021, goal created fertile community conditions for the new delta variant to develop and take root across America. Here we saw the most needless but foreseen consequence of a partisan pandemic: large death tolls in Trump-supporting communities despite a widely available vaccine that was found to be highly effective in preventing death.33
In our concluding chapter, we ask a fundamental question: Could it have been different? Our argument throughout is that a partisan pandemic was not inevitable, but was there any point along the way where the country could have changed course? We argue that with different leadership less focused on an electoral logic along with a more robust public health infrastructure, the outcome could have been different and better. Had the pandemic started in a geographic area more critical to Trump’s reelection campaign, the response from the White House would have likely been more constructive. What do we learn from this pandemic that may help the country navigate the next threat, be it a health scare, a terrorist attack, or climate change? We chart out lessons for policy makers about the importance of having the perspectives of social scientists in helping to shape reactions to health crises. Masks, vaccines, and rapid tests cannot end the pandemic if a substantial portion of the public will not use them. Social scientists can work with public health policy makers to understand how identities such as partisanship can create powerful barriers to uptake.
The COVID-19 death toll is one aspect of the pandemic that we as a nation have yet to fully reckon with. An art installation on the National Mall in Washington, D.C., in September 2021 displayed almost seven hundred thousand white flags, each representing one American lost to the pandemic. As we finish writing this book (in December 2021) that number has surpassed eight hundred thousand, and the pandemic is still our daily reality. The surge of the new omicron variant means that discussion about off-ramps from mask wearing and resuming normalcy have been put delayed once again. The pandemic is not over.
Another part of the pandemic that we have not reconciled is our truly divided country. Partisanship was not merely a political identity; it was a social identity that saved some and killed others. This is why the U.S. pandemic was so unlike the pandemic in other democracies. As our book shows, the partisan divide was set in stone early on and has endured. Across so many attitudes and behaviors, partisanship remains strong and consistent. Partisanship even made the pandemic worse because it politicized every possible solution to COVID-19, from what we wear to how and whether we vote in the next election. And absolutely no solution to a communicable virus will work if it is only adopted by some. The forces that make our political identities strong are the very same that weaken intergroup trust when community needs it the most. With partisan identities more powerful than ever, postpandemic democracy looks more precarious than ever.
The pandemic is still with us. It is represented in the loved ones missing from family dinner tables, the jobs that were never recovered, the symptoms of the so-called COVID long-haulers, the learning setbacks facing an entire generation of children—we could go on. It is also in the guilt and the anger; it is in the mistrust between so-called red people and blue people. We as Americans must understand this pandemic so as to reconcile the past and attempt to move forward together. But it is not something we leave behind. Like the virus, pandemic politics has become endemic too.
This is an excerpt from the book Pandemic Politics: The Deadly Toll of Partisanship in the Age of COVID by Shana Kushner Gadarian, Sara Wallace Goodman, and Thomas B. Pepinsky.
About the Authors
Shana Kushner Gadarian is the Merle Goldberg Fabian Professor of Excellence in Citizenship and Critical Thinking at Syracuse University and the coauthor of Anxious Politics. Sara Wallace Goodman is professor of political science at the University of California, Irvine, and the author of Citizenship in Hard Times. Thomas B. Pepinsky is the Walter F. LaFeber Professor of Government and Public Policy at Cornell University and the coauthor of Piety and Public Opinion.
Notes
1. Taylor Lorenz, Kellen Browning, and Sheera Frenkel, “TikTok Teens and K-Pop Stans Say They Sank Trump Rally,” New York Times, June 21, 2020.
2. Bryan Anderson, Gary D. Robertson, and Jill Colvin, “Trump Says GOP Is Pulling Convention from North Carolina,” Associated Press, June 2, 2020.
3. Jamilah King, “Eight Trump Campaign Staffers Test Positive for Coronavirus after Tulsa Rally,” Mother Jones, June 27, 2020.
4. Sean Murphy, “Health Official: Trump Rally ‘Likely’ Source of Virus Surge,” Associated Press, July 8, 2020.
5. Bert Douglas Bernheim, Nina Buchmann, Zach Freitas-Groff, and Sebastián Otero, “The Effects of Large Group Meetings on the Spread of COVID-19: The Case of Trump Rallies,” Stanford Institute for Economic Policy Research Working Paper No. 20-043, 2020.
6. Ashley Parker and Josh Dawsey, “Seven Days: Following Trump’s Coronavirus Trail,” Washington Post, December 5, 2021.
7. Stephanie Soucheray, “Coroner: First US COVID-19 Death Occurred in Early February,” Center for Infectious Disease Research and Policy, April 22, 2020, https://www.cidrap.umn.edu/news-perspective/2020/04/coroner-first-us-covid-19-death-occurred-early-february.
8. For flu rates, see “Disease Burden of Flu,” Centers for Disease Control and Prevention, January 7, 2022, https://www.cdc.gov/flu/about/burden/index.html.
9. Daniel Carpenter, “Is Health Politics Different?,” Annual Review of Political Science 15, no. 2012 (2012): 287–311.
10. Olivia Waxman, “The Inspiring Depression-Era Story of How the ‘March of Dimes’ Got Its Name,” Time, January 3, 2018.
11. Bethany Albertson and Shana Kushner Gadarian, Anxious Politics: Democratic Citizenship in a Threatening World (New York: Cambridge University Press, 2015).
12. John E. Mueller, “Presidential Popularity from Truman to Johnson,” American Political Science Review 64, no. 1 (1970): 18–34; William D. Baker and John R. Oneal, “Patriotism or Opinion Leadership? The Nature and Origins of the ‘Rally ’Round the Flag’ Effect,” Journal of Conflict Resolution 45, no. 5 (2001):
661–87.
13. Richard C. Eichenberg, Richard J. Stoll, and Matthew Lebo, “War President: The Approval Ratings of George W. Bush,” Journal of Conflict Resolution 50, no. 6 (2006): 783–808.
14. Morris P. Fiorina and Samuel J. Abrams, “Political Polarization in the American Public,” Annual Review of Political Science 11 (2008): 563–88.
15. Jennifer McCoy and Murat Somer, “Toward a Theory of Pernicious Polarization and How It Harms Democracies: Comparative Evidence and Possible Remedies,” Annals of the American Academy of Political and Social Science 681, no. 1 (2019): 235.
16. Marc J. Hetherington, “Resurgent Mass Partisanship: The Role of Elite Polarization,” American Political Science Review 95, no. 3 (2001): 619–31.
17. Ezra Klein, Why We’re Polarized (New York: Simon & Schuster, 2020).
18. Erin C. Cassese, “Straying from the Flock? A Look at How Americans’ Gender and Religious Identities Cross-Pressure Partisanship,” Political Research Quarterly 73, no. 1 (2019): 169–83.
19. Kathy J. Cramer, The Politics of Resentment: Rural Consciousness in Wisconsin and the Rise of Scott Walker (Chicago: University of Chicago Press, 2016).
20. Lilliana Mason, Uncivil Agreement: How Politics Became Our Identity (Chicago: University of Chicago Press, 2018), 14.
21. Gabriel S. Lenz, Follow the Leader? How Voters Respond to Politicians’ Policies and Performance (Chicago: University of Chicago Press, 2013).
22. Julia Azari. “Weak Parties and Strong Partisanship Are a Bad Combination,” Vox, November 3, 2016.
23. Samara Klar, and Yanna Krupnikov, Independent Politics: How American Disdain for Parties Leads to Political Inaction (New York: Cambridge University Press, 2016).
24. Matthew Levendusky, The Partisan Sort: How Liberals Became Democrats and Conservatives Became Republicans (Chicago: University of Chicago Press, 2009); Lilliana Mason, “A Cross-cutting Calm: How Social Sorting Drives Affective Polarization,” Public Opinion Quarterly 80, no. S1 (2016): 351–77.
25. Bernard Berelson, Paul Lazarsfeld, and William McPhee, Voting: A Study of Opinion Formation in a Presidential Campaign (Chicago: University of Chicago Press, 1954).
26. “Writer Michael Anton Makes the Case for Why Trump Should Be Reelected,” National Public Radio, October 20, 2020.
27. Noam Gidron, James Adams, and Will Horne, American Affective Polarization in Comparative Perspective (Cambridge: Cambridge University Press, 2020).
28. Michael Dimock and Richard Wike, “America Is Exceptional in the Nature of Its Political Divide,” Pew Research Center, November 13, 2020, https://www.pewresearch.org/fact-tank/2020/11/13/america-is-exceptional-in-the-nature-of-its-political-divide/.
29. Albertson and Gadarian, Anxious Politics.
30. Leonardo Bursztyn, Aakaash Rao, Christopher Roth, and David Yanagizawa-Drott, “Misinformation during a Pandemic,” NBER Working Paper No. 27417, 2020; Jim Tankersly, Maggie Haberman, and Roni Caryn Rabin, “Trump Considers Reopening Economy, over Health Experts’ Objections,” New York Times, March 23, 2020.
31. Matthew Hartfield and Samuel Alizon, “Introducing the Outbreak Threshold in Epidemiology,” PLOS Pathogens 9, no. 6 (2013): e1003277–e77.
32. Kim Yi Dionne and Fulya Felicity Turkmen, “The Politics of Pandemic Othering: Putting COVID-19 in Global and Historical Context,” International Organization 74, no. S1 (2020): E213–E30.
33. Lena H. Sun and Joel Achenbach, “Unvaccinated People Were 11 Times More Likely to Die of Covid-19, CDC Report Finds,” Washington Post, September 10, 2021.